|
Today's piece is a recap of a recent case referred to VisionAmerica's Dr. Karen Shelton. The goal of this piece is to walk back through a challenging case to see what took place in order to stimulate conversation and learn together. The case is presented and then Dr. Shelton provides her thoughts below. We hope you enjoy it! Your patient presents with the following: A 64-year-old black female is referred for glaucoma evaluation. Past Medical History: HTN, Hypothyroidism, and Arthritis. Family History: Negative for glaucoma IOPs are OD 12 mmHg and OS 13 mmHg at initial visiti and three weeks later were 15 mmHg OU. Pachymetry measured OD 533 and OS 550. 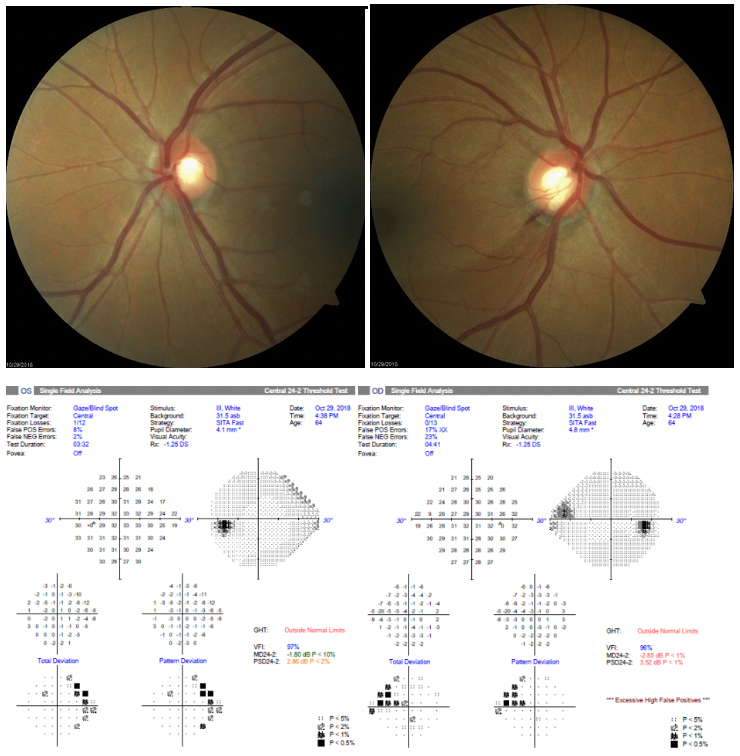  Visual Field - OD shows an apparent nasal step defect and OS shows possible nasal depression versus peripheral artifact. OCT - OD does show a sector of severe RNFL thinning, which would correlate with the superior nasal defect and the RNFL and ONH OS showed normal thickness. Fundus photo - OD also shows an 'Inferior Notch' with drance hemorrhage, which correlates with the superior nasal step. The ONH OS shows a corresponding large cup, but no notching is seen. What would you do? Dr. Karen Shelton: This appears to be a patient with Moderate NTG OD and Mild NTG OS. I typically inquire about any physical symptoms sometimes associated with NTG (e.g. Migraines, Raynauds etc.). I would like to get a couple of IOP measurements at different times of the day. For example, have her come for a morning appointment and the next time have her return in the afternoon. Trying to see if we are able to get any IOP elevation depending on the time of the day. Assuming her average IOP is in the mid-teens, I would still aim to reduce her pressure by 30%. I have found limited success with SLT in these types of cases when the IOP is already low. This is someone that I would prefer to initiate a Monocular trial of a PG analog. Preferably having her start a PG analog in the affected OD first and then if it appears to be efficacious, adding it to the OS. I would then have her return in a month and recheck her IOP. There is a concern that her systemic Ca2+ channel blocker could be causing a decrease in the perfusion of her optic nerve head. This is always a concern when patients have elevated IOP and possibly low BP from medication. This can also be seen in patients with normal IOPs as well. The concern with the patient taking her Ca2+ channel blocker in the morning is that this may be causing her BP to decrease the most in the morning, leading to more difficulty of blood getting into the eye. It may be reasonable to have her try making that change, so she is not taking it in the morning. What would you do if the PG did not reach your target IOP? Dr. Karen Shelton: I would probably add a second medication - either brimonidine or topical CAI. After this, I would probably still give SLT a try before taking the patient to surgery. 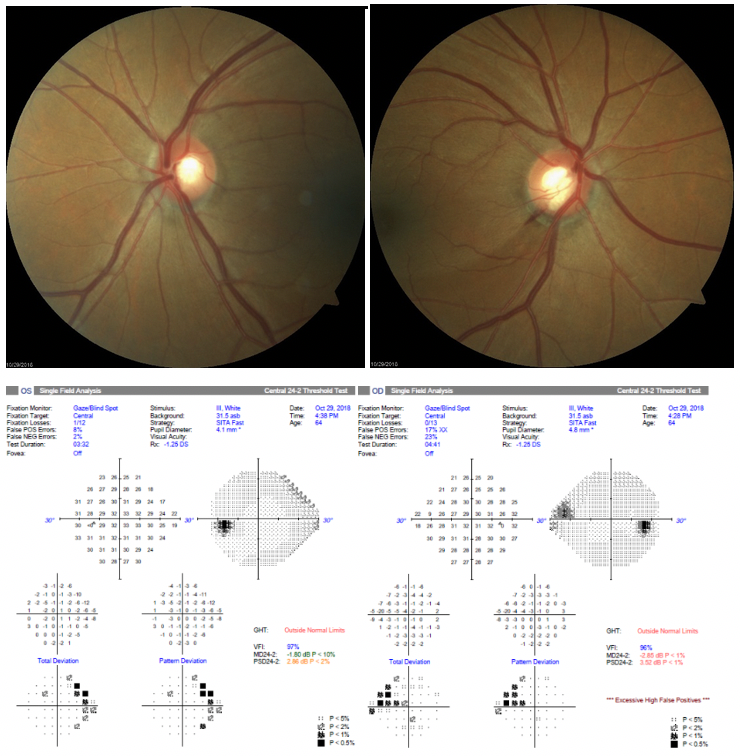
0 Comments
Leave a Reply. |
AuthorThe staff and doctors at VisionAmerica are committed to providing relevant information for you, your patients and your practice. We hope you find the information in our blog post helpful. Archives
August 2019
Categories |
 RSS Feed
RSS Feed
