|
by Paul Batson, O.D. Center Director VisionAmerica of Birmingham Diagnosing and treating a disease like age-related macular degeneration (AMD) is always a challenge. These situations carry quite a bit more weight when the patient is your friend. This case study is a brief summary of my friend's exam history here at VisionAmerica and outlines what our next steps will be. If you have any thoughts or questions on the piece, please send them my way! Case Study 54-year-old friend presents for a second opinion regarding her recent diagnosis of "possible early AMD". Past Medical History - Unremarkable and has never smoked. Base Exam Findings Uncorrected Visual Acuity OD 20/20-1 OS 20/20-2 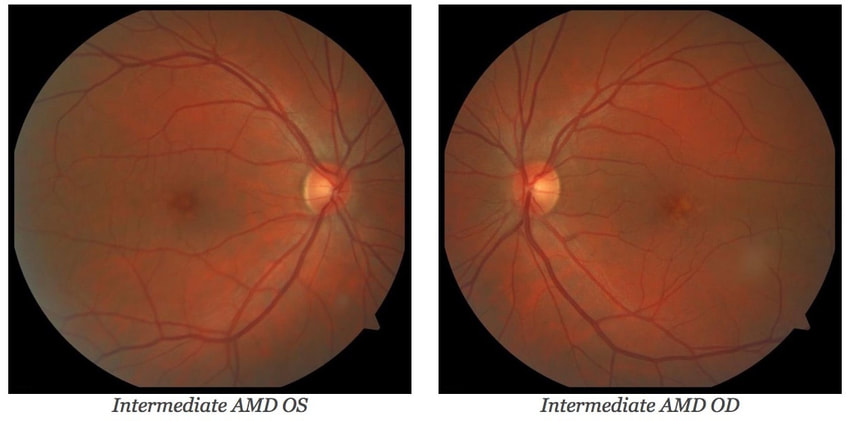 Dilated Fundus Examination - A few hard drusen OU Diagnosis - Macular Drusen OU, No AMD; RTC 1 year 1 Year Follow Up Chief Complaint: Returning for scheduled follow-up of macular drusen, no changes in vision. Past Medical History: No changes Base Exam Findings Uncorrected Visual Acuity OD 20/25-1 OS 20/25-2 Dilated Fundus Examination: Intermediate and Large Drusen (OS>OD) Diagnosis: Intermediate Macular Degeneration Plan: Start AREDS2 Supplements; schedule for genetic testing Discussion: There are a few interesting things to consider for her situation relative to AMD. First, she's a family friend and you all know how those situations can go! Second, she is young, healthy and a non-smoker. In her early 50's, she is rightly concerned about the long-term potential for vision loss and is very anxious and scared. Third, I started her on AREDS2. What if Zinc-related Risk Alleles are true and I potentially make her worse? What concerned me the most was the quick progression from drusen/no AMD to now seeing intermediate-sized drusen in both eyes, along with several large drusen in the left eye. In lieu of her situation and the article published last year by Neely et.al., Prevalence of Undiagnosed Age-Related Macular Degeneration in Primary Eye Care[1], I thought it would be good to remind ourselves and think through a few things related to AMD. If you have not looked at their study, click here. It's a good reminder that we need to cautiously look at these patients. They concluded: "Approximately 25.0% of eyes deemed to be normal based on dilated eye examination by primary eye care physicians had macular characteristics that indicated AMD revealed by fundus photography and trained raters. A total of 30.0% of eyes with undiagnosed AMD had AMD with large drusen that would have been treatable with nutritional supplements had it been diagnosed." I'm personally always looking for those patients that fall in the definition of intermediate AMD because that's the trigger point. According to the Age-Related Eye Disease Study, Early AMD (multiple small drusen, few intermediate drusen (63-124 µm in diameter), or mild RPE abnormalities) like No AMD does not have the evidence to support supplements. But it's still the intermediate AMD patients that I think can sometimes create difficulty defining (and these are, in my opinion, the most important, outside of neovascular membranes). By definition, intermediate AMD includes any of the following features:
So now that I've labeled my friend as Intermediate AMD, I think she now qualifies for AREDS supplements. Technically, AREDS was only evaluated in patients between 55 and 80, but I felt we were close enough. But then I start thinking: She is young and that's potentially a lot of zinc she will be taking over the years. What if the risk alleles within Complement Factor H and ARMS2 genes are true? I could potentially make her vision worse and the reality is that Zinc is not benign. If you'll recall, a group of patients in AREDS that were taking Zinc alone ended up being hospitalized with urinary tract complications. At this point, I've scheduled her with Dr. Nowakowski to test for the risk alleles. I think that I owe it to her to fully inform of all of the data (including what we know and don't know) and let her make the decision. In my recent discussions with Dr. Nowakowski, I will say that the evidence is leaning pretty heavily toward supporting the use of the risk alleles (more on this later). I'll let you know what we find out regarding my friend. [1] JAMA Ophthalmol. 2017;135(6):570-575. doi:10.1001/jamaophthalmol.2017.0830 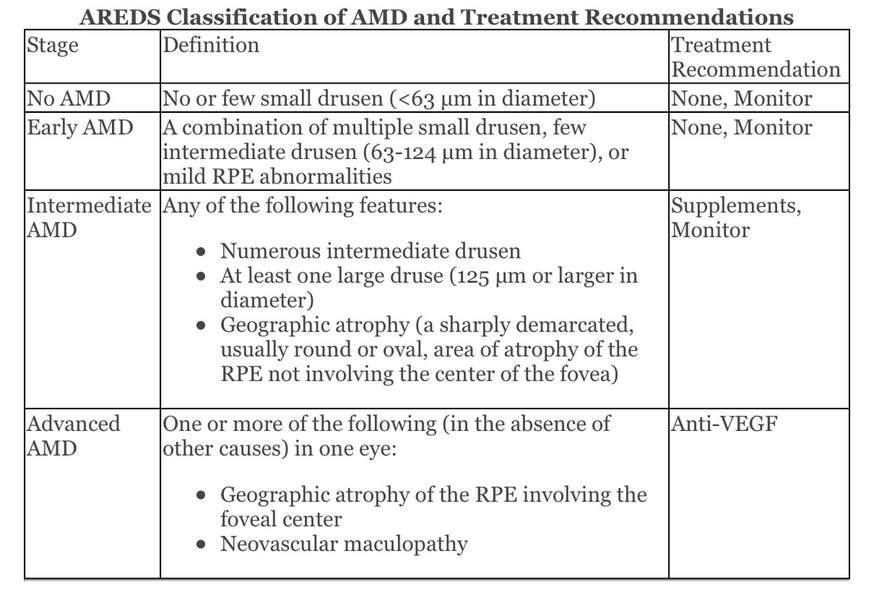
0 Comments
Leave a Reply. |
AuthorThe staff and doctors at VisionAmerica are committed to providing relevant information for you, your patients and your practice. We hope you find the information in our blog post helpful. Archives
August 2019
Categories |
 RSS Feed
RSS Feed
