|
2/7/2018 0 Comments Managing Corneal Ulcers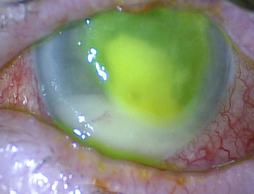 We've all seen them. That patient comes in with their head down and holding their hand over their eye trying to avoid any ray of light. When asked about contact lens wear, they swear they take them out and use fresh solution every night. (To which you want to reply "Liar, Liar".) According to a 2010 CDC report, an estimated 930,000 doctor's office and outpatient clinic visits and 58,000 emergency department visits for keratitis or contact lens disorders occur annually with an estimated direct health care cost of $175 million. We recently sat down with Dr. Matthew Albright, VisionAmerica of Birmingham's corneal specialist to discuss the management of corneal ulcers. What is your approach when it comes to corneal ulcers?
Well, no matter what you may think it is, there is no way of truly knowing. If it is a relatively severe ulcer, then before starting antibiotics of any nature consider the potential need for culturing. Antibiotics will alter and sometimes negate the culture data, which can make therapeutic changes difficult if the initial therapy fails. How do you define severe? Consider how central the lesion is. If it involves the central visual axis (3mm), if it is larger than one millimeter, or if the inflammation is relatively severe. Once treatment begins, how do you recommend monitoring the ulcer? If they respond well, which is noted by a clearing cornea, lessening infiltrate, and less ciliary injection, then that is a clear indication that the antibiotic you have chosen is working. Often, the patient will tell you they are feeling better and seeing better. Reserve judgment on therapeutic improvement for at least 48-72 hours; 24 hours is often not enough time to see a clinical difference. Don't change more than one medicine at a time. This will ensure that you are observing a direct response to your choice of medicine. What is your position on steroids and SCUT (Steroids for Corneal Ulcer Trial)? It is important to consider each patient on a case-by-case basis. The important question to ask is what is my chance of making things worse by adding steroids. If you have started a patient on antibiotics and they have responded well with clear and significant clinical improvement, then it is likely safe to start steroids. If they have not improved on your initial therapy, then you should consider a non-bacterial infection like fungus or acanthamoeba both of which steroids can make worse. If you have any questions about cultures or treating corneal ulcers, please do not hesitate to contact us at (205) 943-4600.
0 Comments
Leave a Reply. |
AuthorThe staff and doctors at VisionAmerica are committed to providing relevant information for you, your patients and your practice. We hope you find the information in our blog post helpful. Archives
August 2019
Categories |
 RSS Feed
RSS Feed
