|
By Trenton Cleghern, OD, FAAO The case study below serves as a good reminder of potential complications that may occur this hot and humid time of year. Chief Complaint A 31-year-old white male presented to our clinic as a follow-up from the eye emergency room with a red and painful left eye. He reported that his symptoms started a few days ago after someone splashed pool water in his eye. The patient was a contact lens wearer and reported excellent lens hygiene and replacement schedule. He was given ofloxacin antibiotic drops at the eye ER to instill every three hours. Base Exam Findings Aided acuities OD: 20/20 OS: 20/50 PH: 20/40 Pupils, EOMs, and CVFs all normal Slit lamp image of the left cornea below. 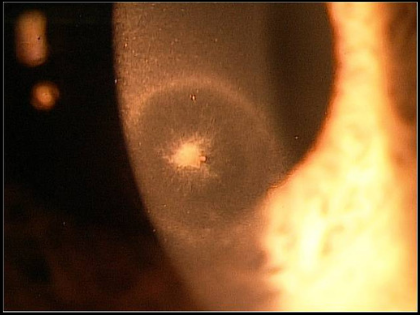 Differential diagnoses included:
Bacterial, herpetic, fungal, and acanthamoeba keratitis. Based on the clinical presentation the patient was diagnosed with fungal keratitis. The infiltrate involved more of the stroma and endothelium. It was not a true ulcer, but did have epithelial disruption. The stroma ring greatly raised suspicion for fungal or acanthamoeba keratitis. With acanthamoeba corneal infections, the stromal ring tends to be more late stage and diffuse, although it can present earlier. The hallmark symptom with acanthamoeba is severe pain that outweighs the clinical signs. This patient had pain, but it was in proportion to the clinical picture. Did the pool water cause this infection or was it just a red herring? We typically think of swimming in contact lenses to be a risk factor of acanthamoeba keratitis. A culture would be helpful, although it can take weeks for fungal isolates to grow on culture media and acathamoeba testing is harder to perform with conventional culture methods. Also, since there was not an epithelial defect, significant epithelial debridement would have to be performed to obtain a culture which could cause more damage than would be helpful. Management The patient was started on natamycin ophthalmic suspension 5% every two hours in the left eye. The ofloxacin was tapered to TID as it was really only for prophylaxis at this point. One drop of atropine was instilled in the left eye. The patient had improvement over the next few weeks. The infiltrate was resolved at one month and the patient's visual acuity had returned to 20/20 in the left eye. Discussion The most common fungal corneal pathogens in the southeastern United States are Aspergillus, Fusarium, and Candida. Aspergillus and Fusarium are more common in patients with vegetative ocular trauma or contact lens abuse. Candida occurs more in immunocompromised patients such as diabetics. Fungal keratitis tends to be a slower and indolent infection than bacteria or herpes simplex. Many of these cases progress to need a penetrating keratoplasty, but that can be avoided with early intervention of topical antifungal therapy and in some cases oral antifungals. Always remember, no steroids on any possible fungal keratitis as this can worsen the condition. These fungal corneal infections come out to play more when the weather is hotter and humid so be on the lookout as we get into summer!
1 Comment
11/6/2023 12:37:57 am
Prescription lenses in existing frames offer a cost-effective eyewear solution. By replacing the lenses in your current frames, you can maintain your preferred style while enjoying clear vision tailored to your prescription. This service is ideal for those who love their frames but require updated lenses. Many optical shops and online providers offer this option, allowing you to customize your eyeglasses according to your specific vision needs without investing in new frames, making it a practical and eco-friendly choice. Leave a Reply. |
AuthorThe staff and doctors at VisionAmerica are committed to providing relevant information for you, your patients and your practice. We hope you find the information in our blog post helpful. Archives
August 2019
Categories |
 RSS Feed
RSS Feed
