 By Trenton Cleghern, OD, FAAO I'm sure we can all remember counting the days to Christmas as a child. We would get out of school for a few weeks and, if we were lucky, get a few good gifts. As adults, things are a bit different. We simply want to escape the office for a few days and enjoy time with friends and family. Few things can be more deflating than some sort of medical problem right before the holidays. Unfortunately, these types of situations happen more often than you would think. As the Christmas holidays approached this past December, an 81-year-old Caucasian female was referred to our office after noticing a "red spot" in her eye and experiencing blurred vision. VisionAmerica's Dr. Trenton Cleghern walks us through the details in our most recent case study. Symptoms
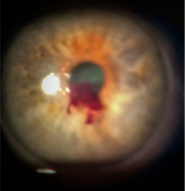
The patient noticed a "red spot" in her right eye that morning. She also experienced some mild blurry vision that cleared when she tilted her head back. The patient also reported that her right eye did not feel normal. Previous History Her past medical history was positive for breast cancer, heart disease, atrial fibrillation with a leaky mitral valve, and hypertension. Her current medications included aspirin, hydrochlorothiazide, losartan, and metoprolol. The patient's ocular history was positive for cataracts OU and dry eye syndrome. Base Exam Findings Her corrected visual acuities were 20/25-1 OD and 20/25+1 OS. Extraocular motilities were full and smooth OU. Pupils were equal, reactive, with no afferent pupillary defect in either eye. Confrontation visual fields were full OU. Her intraocular pressure by Goldmann applanation was 57 mmHg OD and 21 mmHg OS. Anterior segment evaluation of the right eye revealed a blood clot at the inferior pupil margin. The patient also had a corresponding layered hyphema of about five percent. All other findings in the right and left eye were unremarkable except for mild nuclear sclerosis OU. Diagnosis The diagnosis was acute hyphema with ocular hypertension of the right eye. When questioned, the patient reported a vigorous coughing episode the previous night. This, coupled with her aspirin use, was the most likely etiology of her hyphema. Management The patient was given two tablets of 250 mg of acetazolamide orally in the office. One drop of apraclonidine, Simbrinza, and Combigan were also instilled in the right eye. After a short period of time, the intraocular pressure measured 33 mgHg OD. The patient was given samples of Combigan to be used BID OD. She was also prescribed 250 mg tablets of acetazolamide to be taken orally BID. She was also advised to keep her head elevated (even while sleeping) and not to bend over or engage in any rigorous activity or take any additional blood thinners. We did consider stopping her aspirin, but the risk of cardiac complications cannot be taken lightly. When cases like this arise, it is always best to consult with the prescribing physician, but that was not possible here as it was late in the afternoon and right before the holiday weekend. The holiday weekend presented another issue in that our office would not be open until Wednesday of the next week. The patient was scheduled to return to the clinic on that day but was educated thoroughly that if she noticed any decrease in vision, pain, headache, or new ocular symptoms to call our on-call service immediately. Upon follow-up examination five days later, the patient reported no symptoms and that she noticed the blood spot had cleared when she looked in the mirror. Her intraocular pressures were 12 mmHg OD and 15 mmHg OS. Anterior segment evaluation revealed that the hyphema had completely resolved in the right eye. Since there was no sign of any residual blood, all of the glaucoma medications were discontinued. She was advised to resume normal positioning and to follow up with her regular optometrist for an IOP check in three weeks. A rare late-stage complication of hyphema is ghost cell glaucoma. In this scenario, it appears the hyphema has resolved, but actually, the red blood cells have lost their pigment. These depigmented cells can restrict the outflow of the angle and lead to intraocular pressure elevation. This was unlikely due to the rapid resolution of the hyphema, but it was thought prudent to measure the IOP after stopping all of the medications. Discussion/Challenges Managing patients with hyphema usually focuses on two key points: controlling IOP and determining the etiology of the bleeding. It can be obvious, as in this case, with the patient taking a blood thinner and coughing vigorously. Trauma is also a major cause of hyphema, in which a thorough dilated fundus examination should always be performed if possible. In cases where the hyphema is obscuring the fundus view, B-scan ultrasonography is very helpful. When there is no obvious cause, an investigation for a coagulopathy, such as sickle cell anemia, should be initiated. If there is significant inflammation, steroids can be employed, but one must be cautious with potential IOP spikes. Systemic aminocaproic acid was used previously in hospital settings to stabilize bleeding but is rarely used now. Another important point is to advise the patient to keep their head elevated to allow the blood to settle inferiorly. Surgical intervention is reserved for severe cases when IOP cannot be managed medically, the hyphema is severe and not resolving, or corneal blood staining is present. If you have questions for Dr. Cleghern after reading this case study, please do not hesitate to reach out him. Also, as mentioned above, our on-call service can be reached at (205) 943-4600.
0 Comments
Leave a Reply. |
AuthorThe staff and doctors at VisionAmerica are committed to providing relevant information for you, your patients and your practice. We hope you find the information in our blog post helpful. Archives
August 2019
Categories |
 RSS Feed
RSS Feed
